The infant of Mahler’s differentiation subphase of separation-individuation, approx 4-9 months, is observably developed out of total bodily dependence, within a vaguely experienced dual unity with the mother. The infant has a visible “hatched look ” as they start to explore, accumulating discoveries of differences. At the same time, the mother provides continuity and structure, and the infant’s curiosity and excitement are supported by an increasing capacity to move, reach out, and push back. A reciprocal sensitivity between mother and infant, like a mutual cueing, assures a safe, ongoing feedback, supporting growth and separation, the “good enough mother “supports the “going gon being ” of her infant.
The problem with the schizoid personality is that it goes awry, and the infant’s needs and wishes are no longer primary in the dual relationship, but secondary to the mother’s needs. This maternal impingement encourages the infant to develop based on the mother’s needs and demands, and the schizoid sense of self is inhibited via a distorted mirror, based on the mother’s acceptance and availability. The infant relies on the mother to provide continuity of shared experiences to validate and connect to their perceptions. The infant’s broad and spontaneous exploration is curtailed and discouraged, with discrete self-states remaining detached from each other or coming into focus when triggered. This overarching partial state, the false self, is constructed to provide superficial compliance with others; the false self acts as a protector for the true self, whose unacceptable impulses and instincts must remain hidden.
If the mask is removed, there will be no face behind it
The treatment model for the schizoid follows the development model of the “environment – mother, ” who can experience her infant as an entirety, an intuitive being able to hold the infant while they discover themselves. Winnicott’s concept that the transition space is vital, where others are allowed to enter, welcomed, and allowed to play. This space enables the schizoid to test the interpersonal environment. If this is promising, then the next stage is for more intimacy and depth to be possible. The continuous safe relational interaction reduces the fear of anxiety due to spontaneous reaching out based on past persecutory consequences.
Practicing Child
The infant becomes increasingly more upright, more accepting of physical distance from the mother, as long as the child can maintain pleasurable contact by checking back (refuelling). Increased separation remains a delightful experience of discovery of new perceptions as long as refuelling is available. For the practising child (9-15 months), successful passage requires a positive, supportive base that encourages further psychic growth. They need a secure establishment of a rewarding unit (a good part self/good part object) to keep exploring with greater distance. The increasing inner sense of confidence and solidarity will, in turn, slowly begin to admit more negative feelings and a recognition of a non-symbiotic other (not-me). Premature forcing of separateness or acknowledgement of bad feelings may overwhelm the newly cohesive sense of self with a fear of “fragmentation “, overprotectiveness from inevitable faulty starts, and dissatisfaction with practising relationships may tend to entrench concern for and preservation of the status quo. This phase is one of consistency and consolidation, where the child must face the possible anxiety of fragmentation that comes with venturing beyond familiarity and reassurance. The child’s narcissism balances on a developmental edge, tentatively testing a positive sense of selfhood with a trial of the negative, and with it the possibility of separate selfhood.
Rapprochement Phase
The two-year-old of the rapprochement subphase is a negotiating time of major psychological transition. A whole field of differentiated elements must be affirmed and held within an ever-integrating consideration, a balancing and rebalancing as a shifting environment for further thought and action. This is a distinctive developmental challenge, as the child learns to accept oneself and others as separate and individual, which will evoke a mixture of good and bad feelings. Bad feelings might be entertained, with the discovery that they can be rejected or withdrawn from. To disappear to one side of a potential conflict, or assign sides to alternating opposition, no longer works. The toddler may cling to a dependent position because it is associated with good feelings, but it also evokes feelings of personal limitation and a sense of being trapped. The terrible twos are marked by an increasing ambivalence and dissatisfaction in attempting to control a contradictory environment. The mother must demonstrate that mixed feelings are evoked in most situations and must be acknowledged, however conflicting, until they are inclusively considered in terms of both reality and pleasure.
The therapist/mother has the task of remaining steady and consistent in the inconsistent world.
Klein’s concept of the depressive position involves the relinquishing of the idealisation of the mother-child dyad, which is resisted out of fear that acceptance of bad with harm the good, which cannot be repaired. We need to mourn the loss of such idealisation if we are not to remain in melancholy about the necessary acceptance of disillusionment inherent in the human condition. A development of mourning, with the achievement of a conscious, independent, self-observing, and self-correcting self, can now maintain crucial human relationships through a new capacity to perceive the self and others within a deeper complexity. The mother contains the child’s indecision without interfering with the child’s frustration, but improves the child’s capacity to manage it. Mastery of this subphase enables the child to develop the capacity to tolerate mixed impulses within an interpersonal context.
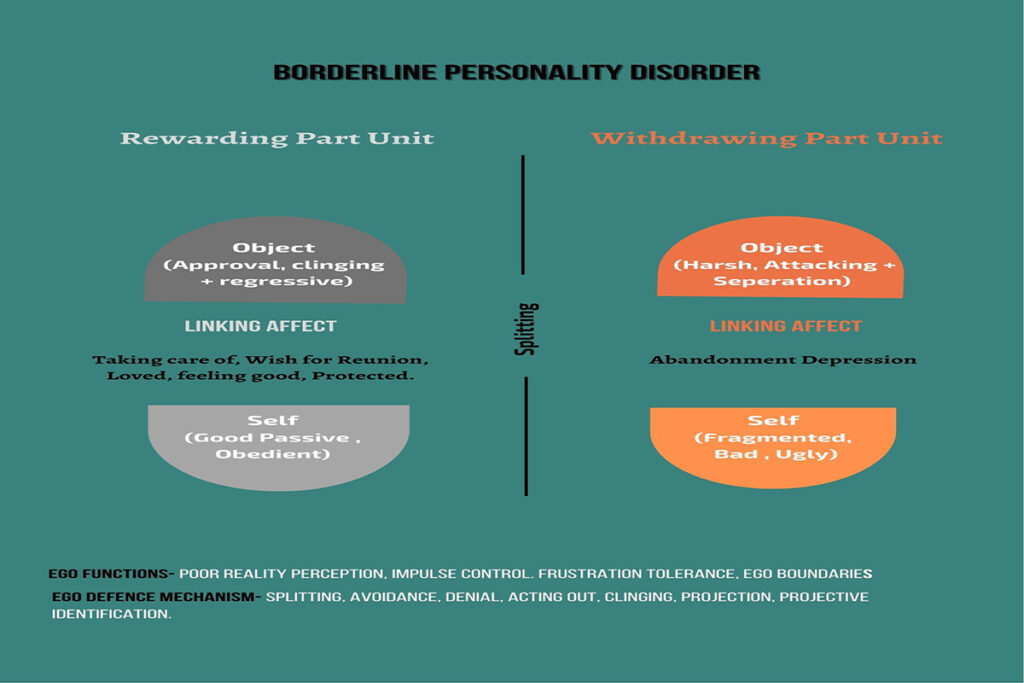
The borderline patient is commonly recognised by changeable moods and states, alternating between clinging and problematic acting out. The BPD child seems to have associated independence with disapproval and dependence with engulfment. The therapist needs to confront the dilemma contained within the independent and dependent stances, to show the contradictory feelings and beliefs. Each achievement of a developmental stage carries the implied threat of the loss of the mother’s love and pushes into the abandonment depression. Without sufficient success of separation and individuation, there cannot be enough definition in the psychic interplay to permit experiencing guilt and reparation (Oedipal Resolution). The borderline client must find the determination not only to face the intense fear of not being able to survive without a mother’s love but also to build enough psychic strength to accept the loss of the ideal in the inner world, which creates a new psychic birth. The pre-object work is a world of absolute opposites; at its most evolved, it is a place of either/or, where self and other, as well as good and bad, are reversed. It understands resolution in terms of win or lose; truce is not moderation, but a pulse in contention. There is success or failure, love or loss. The self and other pick sides, and subjection of one by the other establishes what’s good and moral. Unless irreconcilable opposites can find a resolution in the therapeutic space, there will be no model for new possibilities of arrangements.
The preoedipal mind has not learned fully learned to distinguish the other as apart from the self, to determine gradation of feelings, nor to subject the inner world of wishes and fears to outer experience. Institutions, projections and assumptions are relied upon as much as further definition through specificity and dialectic. This world is governed by either/or thinking that resolves problems by dismissing one extreme, or by oscillating between choices.
Borderline Personality
The client is caught between neurosis and psychosis, usually troubled adolescents, certain impulsivity and unpredictability of mood. The child is expected to grow out of it, where defences sustain the developmental arrest against a profound anxiety of separation and abandonment, depression. The emotional availability of the mother is essential to counterbalance the anxiety evoked in the normal process of separation/individuation. In particular, the mother’s unconditional love for the toddler and her acceptance of ambivalence are crucial. A deep stubbornness to keep protesting, demanding, and repeatedly behaving in self-defeating ways without learning from experience. The psychic unit is composed of 3 elements: the immediate sense of the other, the immediate sense of self, and feeling. Two basic units split the unit.
The Withdrawing – Aggressive Part Unit (WORU)
The rewarding-libidinal part unit (RORU).
Here are the subphases Mahler developed during the separation/individuation process.
Hatching/differentiation – 4-5 months to 9 months
Practising – 9 to 16 months
Rapprochement – 15- 24 months
Object Constancy – 24 months and ongoing.
The borderline is stuck in an unchanging back-and-forth between opposite states, where the client has two alternatives, i.e to feel either bad and abandoned (WORU) or to feel good (RORU) at the cost of denial of reality, arrested growth and self-destructive acting out. Both the clients’ acted out rebellion and acted out clinging must be brought into conscious awareness, where they can be confronted, juxtaposed and integrated within the therapeutic alliance. The client would then have the strength and assurance to face the transformative but devastating feeling that has been warded off; the sense of loss of early and insufficient maternal support that must be exchanged for growing but insecure independence. With consistent confrontations as the client shifts defensive positions, the therapist exemplifies the capacity to hold opposites within an inclusive context. The transformation depends on the therapist’s ability to show the client how one person can contain conflicting perceptions and feelings. This contributes to the client’s perception of a new maternal figure, which can be internalised in the building of a new inner model of self and relationship. The transformation of the rewarding sub-unit from a place of regression to a place for reassurance and reactivation is crucial to the eventual unification of the sub-units.
Narcissistic Personality
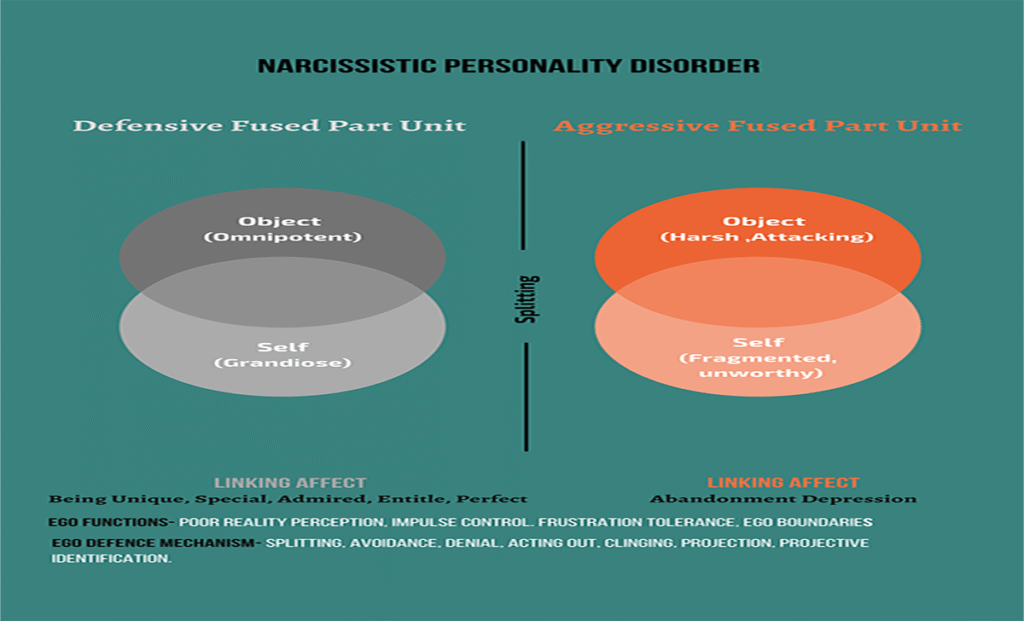
The practising phase is the child’s significant narcissistic involvement in his function and his own body, as well as objects, helping expand his reality. The child’s sense of oneness with an admiring mother prepares for the turmoil of the rapprochement phase. At the end of the preacting stage, there is a clear distinction between self and other, as it begins to dawn on the child that the world is not his oyster, where he must cope with it on his own. one observes the chill sis not ready for this transition and has paused at the time of blissful but illusory importance. The narcissist can be self-confident, even charming when surrounded by admiring others, but without this reassurance, the narc can become dismissive or even hostile. The narc has not been able to establish enough healthy narcissism to sustain the self through realisation of separateness and negative feelings. By dismissal or anger, the narc rejects a disillusioned sense of being “humiliated, attacked, empty “, A fragmentised self that reasserts the defensive self-rep of being grandiose, superior, elite and exhibitionistic.
Secondary narcissism, however, can take on an increasingly regressive nature in the idealisation of the other, whoever possesses an excellence which the ego lacks, for the attainment of the ideal becomes admired. Since the Self /object is a merged representation, the narcissistic transference requires a somewhat fluid state of mind (vicarious intersection) from the analyst. The less differentiated the client’s psyche, the greater the intuitive capacity needed from the analyst. The client appears to be endlessly motivated to seek perfection in all he does, to pursue wealth, power, and beauty, and to find others who will mirror and admire his grandiosity. Underneath the façade lies a state of emptiness and rage, with a predominance of intense envy. The narc can maintain a deceptive appearance as long as the illusion is “borrowed ” from admiring others or adherence to an idealised figure.
Closet Narcissism – inhibited, shy, timid. Ineffective, but has the most elaborate fantasies of grandeur.
Primary narcissism is a blissful state of mind that should be outgrown.
Self-activation leads to anxiety and depression, which leads to defence.
Mirror transference – exuberant feelings of the self-object are weighted toward the child’s sense of self, perceived as a mirror of the self’s grandiosity. The other is expected to serve as the perfect mirror; anything different disrupts the sense of self, which evokes existential anxiety that manifests in abrupt devaluation. When traditional interpretation in therapy is used instead of mirroring, the narcissist feels rebuffed and unprotected from an underlying sense of depletion, may withdraw or lash out.
Idealising Transference – the analyst is placed in an uncomfortable position as the all-knowing, impeccable authority. The narcissist reads a sense of oneness with the analyst’s empathic resonance and validation. The idealising narc often appears subdued and self-effacing, moulding to whom they idealise. A lacklustre life of self-deprecation, compensated for by a dedication to the rules, morals, and institutions that govern him, has led to disillusionment, perhaps stemming from a fall from grace or a steady erosion of unquestioning devotion to the community. The client is beset by a dim feeling, not so much depression as a troublesome sense of incompleteness.
Alter Ego / Twinship – experienced a being like the grandiose self or very similar to it. The analyst thinks like me, shares my perspective, and has the same perceptions as I do.. A stable psychic ground is established to support a growing sense of self in a “fractional way “. Through the analyst’s continued empathy, the transmutation of internalisation of maternal repression facilitates a strengthening of the ego and the beginning of separation from others without fragmentation.
Abandonment Depression
The client has an unconscious need to replicate the decisive moment in early growth, where the mother consistently withdrew her libidinal availability in response to her child’s expressions and excitement. This negative maternal response was sufficient to motivate complaint activity (or inactivity) to ensure loving care (survival) from the mother. This feeling of imminent loss and profound alarm is repeatedly evoked with each therapeutic challenge to the dysfunctional defences that hold back the natural emergence of the self. Increasing self-activation means trusting uncertainty and the unknown, trusting a new personality pattern and suffering the loss of an old structure that sustained the self. The resultant “Abandonment Depression ” for fear of self-assertion has evoked retributive maternal loss, a predictable regression where clients move closer to healing, especially near termination. Workable resistance to psychic changes presents itself in self-sabotaging behaviour. To work through the abandonment depression, the developmental arrest, in the narc client, that inhibits constructive growth, is resolved. What differentiates the closeted narcissist from other personality disorders is the experience of abandonment depression as the self falling apart, fragmenting rather than losing the love object. It’s necessary to work through this fragmentation anxiety to progress developmentally once the self has gained enough strength to do so. The initial terror of maternal /self loss, which had overwhelmed and defensively frozen one’s development, must be faced within the therapeutic alliance to restore psychological growth.
Schizoid Personality
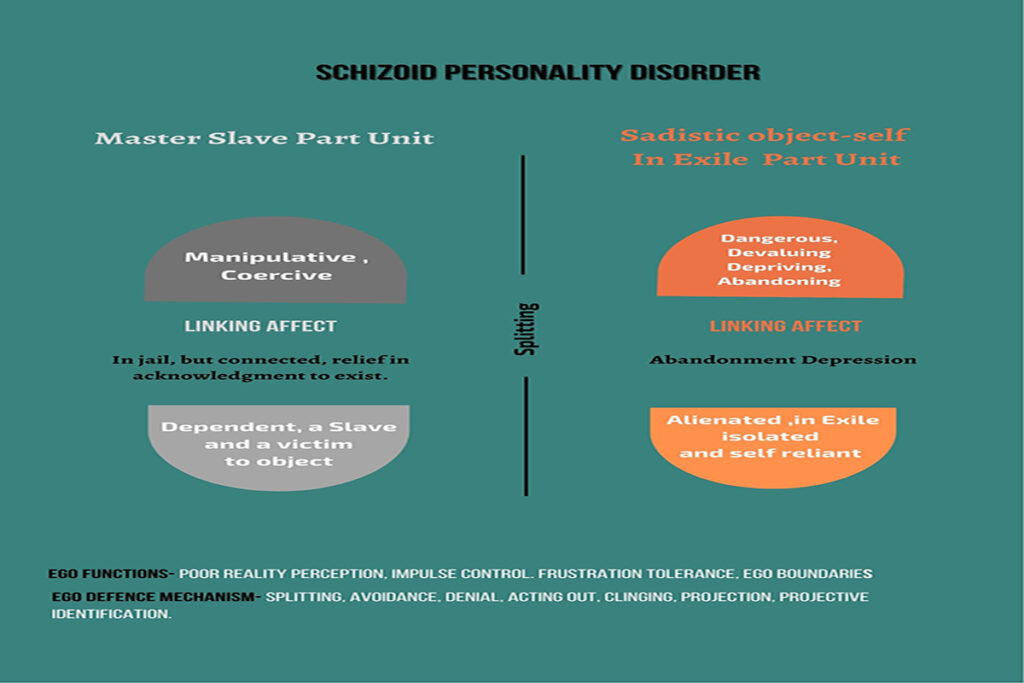
A character pathology originating from maternal devaluing of the self, leading to emotional detachment and social withdrawal. A closed system protected from outside encroachment, but constantly subject to a painful inner sense of futility. How does the child learn to love without destroying love? The child becomes afraid of love and intimacy, erecting barriers between himself and others. There is a need to regulate interpersonal distance and accompanying persuasive tension between the need for attachment. Emotional deprivation in early childhood creates fantasies of a ravenous devouring and destruction of the source of sustenance ( mother). The isolated schizoid longs for a relationship and approaches it with guarded behaviour. As he draws close, he experiences fear of old pain of failure and hurt and withdraws again into his private safe world.
Faulty adaptation of the child within the maternal environment results in an impairment of self and a sense of safety/self retained in isolation. The true self, one of spontaneous impulse and instinctual life, goes into hiding, and a false self is formed in compliance with the impinging environment. The good-enough mother’s holding stance supports the child’s aliveness, creativity, and curiosity. The false self is a defensive construct formed to minimise the psychic pain of having to recognise and adjust to maternal misattunement. The schizoid client tends to be a notably “unhatched” interpersonal standoff, where the therapist attempts to make contact but encounters a discouraging lack of response, a flattened, detached, and withdrawn manner. A terrifying fear of non-existence and a deep sense of estrangement result from the experience of having to forgo one’s true self, having to live reactively and respond to the needs, expectations, and intrusions of others.
The resolution lies in the client’s ability to face the terror underlying any attempt to be; the dreaded possibility that one is not even there to begin with. To face the experience of unfreezing the familiar situation, where the true self was denied, and to gain sufficient strength to act on their convictions of self-belief, sufficiently overcoming traumatised fear and trust in a rebirth of the self. Intensive long-term therapy is a dynamic, reparative process that endeavours to help the schizoid client’s ability to face the primal anxiety of non-relatedness (abandonment depression). The resolution of a traumatic block is the successful mastery of an early developmental task that allows the client to accept a fundamental internal need for relatedness.
This challenging work requires restructuring, an actual rebirth of the self.
The six abandonment feelings that make up this psychological onslaught are: depression, anger and rage, fear, guilt, passivity and helplessness, emptiness and void. These are the feelings that arise from the loss or threat of losing either part of the self or supplies the client believes are vital for survival. Such feelings may be challenging to face if the client is to resolve the long-standing dread of loss of a mother’s nurturing, which caused the early developmental arrest. As defences are successfully interrupted, the depression becomes more intense, repressed memories emerge, and the client is suffering. The suffering/anxiety is characterised as a fear of annihilation (schizoid), fear of fragmentation (narc ), collectively referred to as abandonment depression. The depressive position fades with a maturing desire for reparation and capacity for concern. Unless the client can achieve a capacity to mourn, to let go of idealisation and accept the often complex conflict of reality, the passage to ordinary neurosis is doubly hazardous for the borderline. The object, especially as the split closes, is perceived as a unique, specific person. Responsibility for going on being can now be transferred from the other to the self.
Orcutt, C. (2021). The Unanswered Self: The Masterson Approach to the Healing of Personality Disorder. The Masterson Approach to the Healing of Personality Disorders , Karnac Books
The narcissistic child has omnipotent, controlling and tyrannical fantasies of controlling his mother (object), which are part of normal development but need to be...